Uterine Fibroids Treatment in Newport Beach — Myomectomy vs Hysterectomy Decision Guide (2026) | Broad Medical Group
(949) 720-9848
Uterine Fibroids · Newport Beach · 2026
Uterine Fibroids Treatment Types, Symptoms & the Surgical Decision
Understanding your fibroids. Knowing your options. Making the right choice for your body.
Uterine fibroids are the most common benign tumors of the female reproductive tract,
but not every fibroid needs treatment. This guide covers fibroid types and their clinical
significance, when treatment is warranted, the full range of options from observation
to surgery, and the critical decision between myomectomy and hysterectomy —
including what matters most for fertility.
Uterine fibroids (leiomyomas) are benign smooth muscle tumors that
affect up to 70–80 percent of women by age 50, though only
about 25 percent become symptomatic ACOG PB #228. The most
common symptom is heavy menstrual bleeding, which can lead to iron
deficiency anemia. Treatment depends on symptom severity, fibroid location and size,
and the patient’s reproductive goals. Asymptomatic fibroids
require only periodic monitoring. When treatment is needed, options range from
medical management (hormonal therapy, tranexamic acid) to
procedural interventions (uterine artery embolization) to
surgery. The central surgical decision is myomectomy
(fibroid removal, uterus preserved) versus hysterectomy (definitive
treatment) ACOG PB #228; ACOG CO #701. Neither is inherently
superior — the right choice depends on the patient’s goals, particularly
regarding fertility and uterine preservation. Malignant transformation is
extremely rare (<0.1%)Stewart 2015. At Broad Medical Group,
Dr. Jennifer Broad provides individualized fibroid evaluation
and treatment for patients in Newport Beach and Orange County.
Medically reviewed by Dr. Jennifer Broad, MD, FACOGBoard-Certified Obstetrician-Gynecologist · Newport Beach, CA
Last reviewed: April 2026Next review: October 2026
What Are Uterine Fibroids?
Uterine fibroids — also called leiomyomas or simply
myomas — are benign (non-cancerous) tumors that arise from
the smooth muscle cells of the uterine wall. They are the most common pelvic tumors
in women of reproductive age, affecting an estimated 70 to 80 percent of
women by age 50. Despite this extraordinary prevalence, only about
25 percent of women develop symptoms significant enough to seek
medical care.
Fibroids range in size from tiny seedlings invisible to the naked eye to large masses
that can distort the uterus to the size of a full-term pregnancy. They can be single
or multiple — it is common to find several fibroids of varying sizes in the
same uterus. Their growth is driven primarily by estrogen and progesterone, which
is why fibroids typically develop during the reproductive years and tend to shrink
after menopause when hormone levels decline.
The exact cause of fibroids remains incompletely understood, but risk factors include
age (peak incidence in the 40s), African American race
(2–3 times higher incidence and earlier onset), family history,
obesity, and nulliparity (never having given birth).
Early menarche (first period before age 10) is also associated with increased risk.
Key Fact
Fibroids are not cancer. Malignant transformation of a fibroid into
a uterine sarcoma (leiomyosarcoma) is extremely rare — less than 0.1
percent. When uterine sarcomas are found, the current evidence suggests they
arise independently rather than from degeneration of existing fibroids. The presence
of fibroids should not create fear of cancer. However, any fibroid with unusual
characteristics on imaging or rapid, unexplained growth warrants further evaluation.
Fibroids are managed within the broader context of gynecologic care, and when surgery
is indicated, modern approaches favor minimally invasive techniques. For details on
surgical approaches, technology, and recovery expectations, see our
minimally invasive gynecologic
surgery guide.
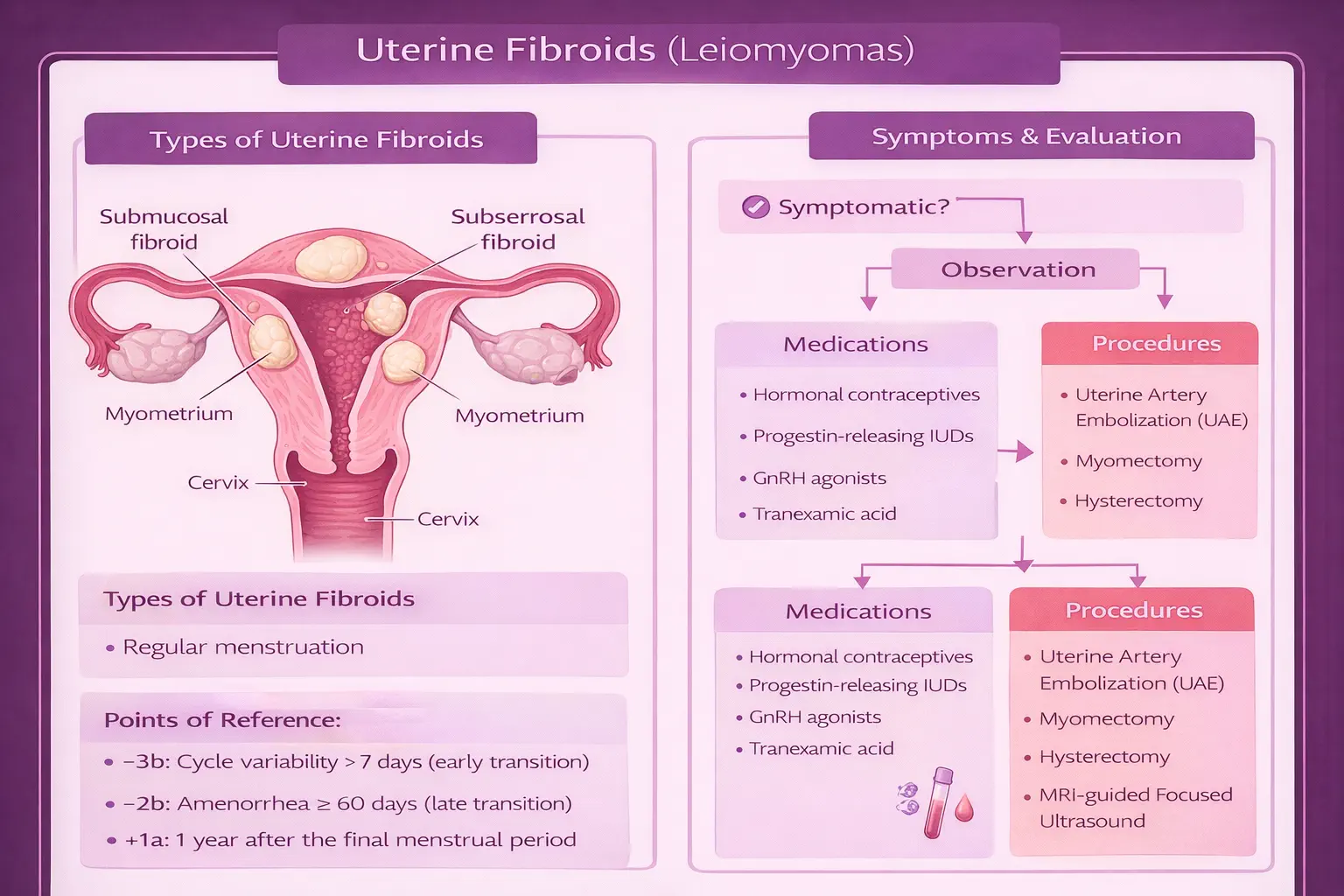
Types by Location
ACOG PB #228FIGO Classification
The clinical significance of a fibroid depends more on where it is located
than on its mere presence. A 2-centimeter submucosal fibroid distorting the uterine
cavity can cause debilitating heavy bleeding and infertility, while a 6-centimeter
subserosal fibroid may cause no symptoms at all. This is why classification by
location is essential for treatment planning.
The FIGO (International Federation of Gynecology and Obstetrics) classification
system categorizes fibroids from type 0 through type 8 based on their
relationship to the uterine cavity, myometrium, and serosal surface. In clinical
practice, the four primary location categories are:
Type
Location
Primary Symptoms
Submucosal
Projects into the uterine cavity (FIGO 0–2)
Heavy menstrual bleeding, infertility — most symptomatic relative to size
Intramural
Within the uterine muscle wall (FIGO 3–5)
Heavy bleeding, pelvic pressure, bulk symptoms — most common type
Subserosal
Outer surface of the uterus (FIGO 6–7)
Pelvic pressure, bladder or bowel compression — may be asymptomatic
Pedunculated
Attached to uterus by a stalk (submucosal or subserosal)
Torsion risk (acute pain), pressure symptoms, or cavity distortion
FIGO classification of uterine fibroids by location. Submucosal fibroids cause the most symptoms relative to their size because they distort the uterine cavity.
In practice, many women have fibroids in multiple locations
simultaneously. A patient might have a large intramural fibroid causing bulk
symptoms alongside a small submucosal fibroid causing heavy bleeding. The
treatment plan must account for the entire fibroid burden, not just the largest
or most obvious fibroid. Pelvic ultrasound is the first-line imaging study;
MRI provides superior detail when surgical planning requires precise mapping
of fibroid number, size, and location.
Symptoms: When Fibroids Become a Problem
It bears repeating: most fibroids are asymptomatic. Many women
learn they have fibroids incidentally — during a routine pelvic exam or an
ultrasound performed for another reason — and never experience a single
symptom. However, when fibroids do cause symptoms, those symptoms can range from
mildly annoying to severely life-disrupting.
Heavy Menstrual Bleeding (Menorrhagia)
This is the most common symptom of uterine fibroids. Submucosal
and large intramural fibroids disrupt the normal contractile ability of the uterine
muscle and increase the surface area of the endometrial lining, both of which
contribute to heavier and prolonged menstrual flow. Women with fibroid-related
menorrhagia often describe periods lasting 7–10 days or longer, soaking
through a pad or tampon every hour, passing large blood clots, and needing to
use double protection (pad and tampon simultaneously).
Iron Deficiency Anemia
Chronic heavy menstrual bleeding leads to iron deficiency anemia
— a condition in which the body’s iron stores are depleted faster than
they can be replenished. Symptoms of anemia include fatigue, weakness, shortness
of breath with exertion, lightheadedness, and difficulty concentrating. Many women
attribute these symptoms to stress or aging rather than recognizing them as a
consequence of their heavy periods. Anemia related to fibroid bleeding is one of
the clearest indications that treatment — not continued observation —
is warranted.
Pelvic Pressure and Bulk Symptoms
Large fibroids, particularly subserosal and intramural types, can cause a sensation
of pelvic fullness, heaviness, or pressure. Depending on the fibroid’s position,
bulk symptoms include:
Urinary frequency or urgency — fibroid compressing the
bladder, reducing its capacity
Difficulty emptying the bladder completely — obstruction
of the urethra or bladder neck
Constipation — fibroid compressing the rectum
Lower back pain — large posterior fibroids pressing on
spinal nerves
Abdominal distention — very large fibroids (or a
significantly enlarged uterus) causing visible enlargement of the abdomen
Pain
Fibroids are not typically painful in the way that endometriosis is painful, but
pain can occur in specific scenarios: degeneration (when a fibroid
outgrows its blood supply and the tissue begins to break down, causing acute pain),
torsion of a pedunculated fibroid (the stalk twists, cutting off
blood flow — this is a surgical emergency), and dysmenorrhea
(painful periods associated with large intramural fibroids).
Infertility
Submucosal fibroids that distort the uterine cavity are most clearly
associated with reduced fertility and increased miscarriage risk. The distortion
interferes with embryo implantation and early pregnancy maintenance. This topic
is discussed in detail in the fibroids and fertility
section below.
Patient Tip
Track your symptoms before your appointment. A menstrual diary
— recording the duration of your period, the number of pads or tampons used
per day, whether you pass clots, and any associated pain or pressure — gives
Dr. Broad objective data to assess the severity of your symptoms and guide
treatment decisions. Two to three cycles of tracking is ideal.
Do Fibroids Need Treatment?
Not every fibroid needs treatment. This is one of the most important
points to understand. The presence of fibroids on an ultrasound report does not
automatically mean you need surgery, medication, or any intervention at all.
The decision to treat is driven by symptoms and their impact on quality
of life, not by the mere existence of fibroids.
The following framework guides treatment decisions:
Observation (No Treatment)
Asymptomatic fibroids are managed with periodic monitoring,
typically an annual pelvic exam and ultrasound to track size and growth. Many
women live their entire lives with fibroids that never require intervention.
After menopause, declining estrogen levels often cause fibroids to shrink
on their own.
When Treatment Is Indicated
Symptoms affect quality of life — heavy bleeding that
disrupts daily activities, pelvic pressure that interferes with exercise or
daily function, or urinary symptoms that affect sleep
Causing iron deficiency anemia — chronic heavy bleeding
has depleted iron stores to the point where the patient is symptomatic or
laboratory values are abnormal
Contributing to infertility — specifically, submucosal
fibroids distorting the uterine cavity in a woman trying to conceive
Rapid growth raises concern — while rapid growth alone
is not diagnostic of malignancy, a fibroid that increases significantly in
size over a short period warrants further evaluation with imaging (typically
MRI) and clinical discussion
Important
Rapid growth of a fibroid warrants evaluation, not panic.
While uterine sarcoma (leiomyosarcoma) is extremely rare, rapid or unexpected
growth — particularly in a postmenopausal woman when fibroids should be
shrinking — is a reason to pursue further imaging and possibly tissue
diagnosis. This is a conversation to have with your gynecologist, not a reason
to assume the worst.
Treatment Options: The Decision Framework
When fibroid symptoms warrant treatment, the options span a spectrum from
medical management to minimally invasive procedures to surgery. The right
approach depends on the patient’s age, symptom severity, desire for
fertility, fibroid characteristics (number, size, location), and personal
preference. There is no single “best” treatment — there is
the best treatment for you.
A. Observation (Watchful Waiting)
As discussed above, asymptomatic fibroids do not require treatment. Monitoring
with periodic pelvic exam and ultrasound is the appropriate management. This is
not “doing nothing” — it is an active decision supported by
evidence that most fibroids never require intervention.
B. Medical Management
Medical therapy does not eliminate fibroids. It controls symptoms,
primarily heavy bleeding, while avoiding or delaying surgical intervention.
Options include:
Hormonal contraceptives (combined oral contraceptive pills,
progestin-only pills, hormonal IUD) — reduce menstrual bleeding and
cramping. The levonorgestrel IUD (Mirena) is particularly effective for
bleeding reduction in women with fibroids, though it does not shrink them.
GnRH agonists (leuprolide/Lupron) — create a temporary
medically induced menopause, causing fibroids to shrink by 30–50 percent.
Used primarily as preoperative therapy for 3–6 months
before myomectomy to reduce fibroid size, decrease blood loss at surgery, and
correct anemia. Not suitable for long-term use due to bone density loss and
menopausal side effects.
GnRH antagonists (elagolix/Oriahnn, relugolix/Myfembree)
— newer oral medications that reduce heavy menstrual bleeding associated
with fibroids. Unlike GnRH agonists, they are combined with low-dose hormonal
add-back therapy to minimize bone loss and menopausal symptoms, allowing
longer-term use (up to 24 months in clinical trials).
Tranexamic acid (Lysteda) — a non-hormonal antifibrinolytic
agent taken during menstruation to reduce heavy bleeding. It does not affect
fibroid size or hormonal status. A reasonable option for women who want to
avoid hormonal therapy.
Iron supplementation — not a treatment for fibroids,
but an essential component of management when heavy bleeding has caused anemia.
Oral iron or, in severe cases, intravenous iron infusion may be needed to
restore iron stores before surgery.
C. Procedural Interventions
These approaches fall between medical management and surgery:
Uterine artery embolization (UAE) — a minimally invasive
procedure performed by an interventional radiologist. Small particles are
injected into the uterine arteries to block blood flow to the fibroids,
causing them to shrink over the following months. UAE preserves the uterus
and avoids the recovery of open surgery. However, UAE is generally
not recommended for women who desire future pregnancy, as its effects
on uterine blood flow and ovarian reserve are not fully established.
Potential complications include post-embolization syndrome (pain, fever,
nausea) and, rarely, premature ovarian insufficiency.
MRI-guided focused ultrasound (MRgFUS) — uses
high-intensity focused ultrasound waves guided by MRI to heat and destroy
fibroid tissue. Non-invasive (no incision), but limited availability,
strict size and number restrictions (typically a single fibroid <10cm), and
variable long-term outcomes limit its use. Not widely recommended as a
first-line option.
D. Surgical Treatment
When fibroids require definitive intervention, the surgical decision centers on
two procedures: myomectomy and hysterectomy.
Myomectomy removes the fibroids while preserving the uterus.
The surgical approach depends on fibroid characteristics:
Hysteroscopic myomectomy — for submucosal fibroids
(FIGO 0–1, some type 2). A camera is passed through the cervix into
the uterine cavity; no abdominal incision. The fibroid is resected from
inside the uterus. Outpatient procedure with rapid recovery.
Laparoscopic myomectomy — for subserosal and intramural
fibroids that are accessible laparoscopically. Small abdominal incisions,
minimally invasive, faster recovery than open surgery. May be performed with
robotic assistance.
Open (abdominal) myomectomy — for very large fibroids,
a large number of fibroids, or fibroids in locations not safely accessible
laparoscopically. Requires a larger abdominal incision (similar to a cesarean
section) and longer recovery.
Hysterectomy removes the uterus and is the only treatment that
guarantees fibroids will not recur. ACOG Committee Opinion No. 701 recommends
that when hysterectomy is indicated, a minimally invasive approach
(laparoscopic or vaginal) should be used whenever feasible. Open
abdominal hysterectomy should be reserved for cases where minimally invasive
approaches are not safe or appropriate. For details on surgical approaches and
recovery expectations, see our
minimally invasive
surgery guide.
Clinical Illustration â€" Treatment decision flowchart: Asymptomatic (observe) vs Symptomatic (medical management first, then procedural or surgical based on fertility goals and fibroid characteristics)
Fibroid treatment decision framework. The pathway from observation to intervention depends on symptoms, reproductive goals, and fibroid characteristics.
Myomectomy vs Hysterectomy: The Decision
This is the decision that most patients find most difficult, and it is the one
that Dr. Broad spends the most time discussing. Both myomectomy and
hysterectomy are effective treatments for symptomatic fibroids, but they represent
fundamentally different approaches with different implications.
Neither procedure is “better.” The right choice depends
entirely on the patient’s circumstances, values, and goals. Dr. Broad’s
role is to ensure you understand both options completely so you can make a
decision that aligns with your life.
When Myomectomy Is Preferred
Fertility is desired — myomectomy preserves the uterus,
making future pregnancy possible
Patient wants uterine preservation — for personal,
cultural, or psychological reasons, independent of fertility goals
Fibroids are surgically accessible — number, size,
and location are amenable to complete removal
Patient accepts the possibility of recurrence —
fibroid recurrence after myomectomy is approximately 15 to 30
percent within 5 years, meaning that a second procedure may
eventually be needed
When Hysterectomy Is Preferred
Childbearing is complete — no future pregnancies
are desired
Recurrent fibroids after prior myomectomy — the
patient has already undergone fibroid removal but new symptomatic fibroids
have developed
Coexisting adenomyosis — a condition in which
endometrial tissue grows into the uterine muscle wall, causing pain and
heavy bleeding that myomectomy cannot address
Patient prefers definitive treatment — wants the
certainty that fibroids will not recur
Massive or numerous fibroids — the uterus is so
heavily affected that myomectomy would leave inadequate uterine tissue
or carry unacceptable surgical risk
Recurrence After Myomectomy
One of the most important counseling points is that myomectomy is not necessarily
a permanent solution. Studies report that 15 to 30 percent of women
will develop new fibroids or experience growth of residual fibroids within
5 years of myomectomy. The recurrence rate is higher when
multiple fibroids were present at the time of surgery. Some women with recurrence
remain asymptomatic, while others may eventually require a second myomectomy
or proceed to hysterectomy.
This is not a reason to avoid myomectomy — it is a reason to go into the
decision with realistic expectations. For women who need uterine preservation,
myomectomy is the right choice even knowing that future intervention may be needed.
ACOG Guideline
ACOG Committee Opinion No. 701 recommends that minimally
invasive hysterectomy (laparoscopic, robotic-assisted, or vaginal) should
be performed whenever feasible, as it is associated with shorter hospital stays,
fewer complications, less postoperative pain, and faster return to normal activity
compared to open abdominal hysterectomy. The same minimally invasive principles
apply to myomectomy when fibroid characteristics permit.
Fibroids and Fertility
The relationship between fibroids and fertility is nuanced. Not all fibroids
affect the ability to conceive or carry a pregnancy — the critical factor
is whether the fibroid distorts the uterine cavity.
Which Fibroids Affect Fertility?
Submucosal fibroids (cavity-distorting) — the strongest
evidence links submucosal fibroids to reduced conception rates and increased
miscarriage risk. These fibroids alter the endometrial surface where embryo
implantation occurs, and may disrupt the normal vascular and biochemical
environment needed for early pregnancy.
Large intramural fibroids (>4cm) — may affect
fertility even without directly protruding into the cavity, particularly when
they distort the uterine contour or obstruct the fallopian tube ostia.
The data are less definitive than for submucosal fibroids, but many
reproductive endocrinologists consider removal when intramural fibroids
exceed 4 centimeters in a woman with otherwise unexplained infertility.
Subserosal fibroids — on the outer surface of the
uterus. Generally do not affect fertility unless they are
very large and causing significant compression or distortion.
Does Removing Fibroids Improve Pregnancy Rates?
For cavity-distorting fibroids, the evidence supports removal.
Studies consistently show that removing submucosal fibroids via hysteroscopic
myomectomy improves pregnancy rates and reduces miscarriage rates. For intramural
fibroids, the evidence is more mixed but suggests benefit when fibroids are large
(>4cm) or when no other cause of infertility is identified.
Planning: From Myomectomy to Conception
When myomectomy is performed for fertility purposes, the typical timeline is:
Myomectomy — performed via hysteroscopy (submucosal)
or laparoscopy/laparotomy (intramural)
Waiting period — typically 3 to 6 months
after surgery before attempting conception, to allow the uterus to heal fully.
The waiting period is longer for open or laparoscopic myomectomy (where the
uterine wall was entered) than for hysteroscopic myomectomy.
Conception attempts — natural or assisted (IVF) as
appropriate for the patient’s overall fertility picture
Delivery After Myomectomy
Whether a cesarean delivery is recommended after myomectomy depends on the
depth of myometrial entry during the surgery. If the myomectomy
involved a deep incision into the uterine wall (particularly a full-thickness
entry into the uterine cavity), most providers recommend cesarean
delivery due to the theoretical risk of uterine rupture during labor.
Hysteroscopic myomectomy, which does not involve incision through the outer
uterine wall, does not typically require cesarean delivery. This is discussed
with each patient at the time of myomectomy so that delivery planning can
begin early.
Key Takeaways
Uterine fibroids affect up to 70–80% of women by age 50, but only about 25% become symptomatic. They are benign, and malignant transformation is extremely rare (<0.1%).
Location determines clinical significance — submucosal fibroids cause the most symptoms relative to size; subserosal fibroids may cause none at all.
Not every fibroid needs treatment. Asymptomatic fibroids are monitored with periodic exams and imaging. Treatment is driven by symptoms and quality of life, not by size alone.
Medical management controls symptoms but does not eliminate fibroids. Hormonal therapies, GnRH agonists/antagonists, and tranexamic acid are first-line for bleeding control.
The central surgical decision is myomectomy vs hysterectomy. Myomectomy preserves the uterus (and fertility) but carries 15–30% recurrence within 5 years. Hysterectomy is definitive.
Submucosal fibroids have the clearest impact on fertility. Removal of cavity-distorting fibroids improves pregnancy rates. After myomectomy, a 3–6 month waiting period before conception is typical.
ACOG recommends minimally invasive approaches for both myomectomy and hysterectomy when feasible, with faster recovery, fewer complications, and less postoperative pain.
References & Clinical Sources
American College of Obstetricians and Gynecologists. Practice Bulletin No. 228: Management of Symptomatic Uterine Leiomyomas. Obstetrics & Gynecology, 137(6), e100–e115. 2021.
American College of Obstetricians and Gynecologists. Committee Opinion No. 701: Choosing the Route of Hysterectomy for Benign Disease. Obstetrics & Gynecology, 129(6), e155–e159. 2017. Reaffirmed 2021.
Donnez J, Dolmans MM. Uterine fibroid management: from the present to the future. Human Reproduction Update, 22(6), 665–686. 2016.
Stewart EA. Uterine fibroids. New England Journal of Medicine, 372(17), 1646–1655. 2015.
AAGL Practice Report: Practice Guidelines for the Diagnosis and Management of Submucous Leiomyomas. Journal of Minimally Invasive Gynecology, 19(2), 152–171. 2012.
Pritts EA, Parker WH, Olive DL. Fibroids and infertility: an updated systematic review of the evidence. Fertility and Sterility, 91(4), 1215–1223. 2009.
Living with fibroid symptoms or facing a treatment decision? Dr. Broad provides
individualized fibroid evaluation — from initial imaging through treatment
planning and surgical care — for patients in Newport Beach and Orange County.
Medical Disclaimer: This content is for educational purposes only and does not
constitute medical advice, diagnosis, or treatment. Consult Dr. Jennifer Broad or your healthcare
provider for guidance specific to your situation. Current as of April 2026.
If you are experiencing a medical emergency, call 911 immediately.
This site uses cookies for analytics to improve your experience. Privacy Policy · Opt-Out