Menopause & HRT · Newport Beach · 2026 Edition
Menopause & Hormone Replacement Therapy
Evidence-Based Treatment Guide
Not guesswork. Not marketing. Clinical evidence.
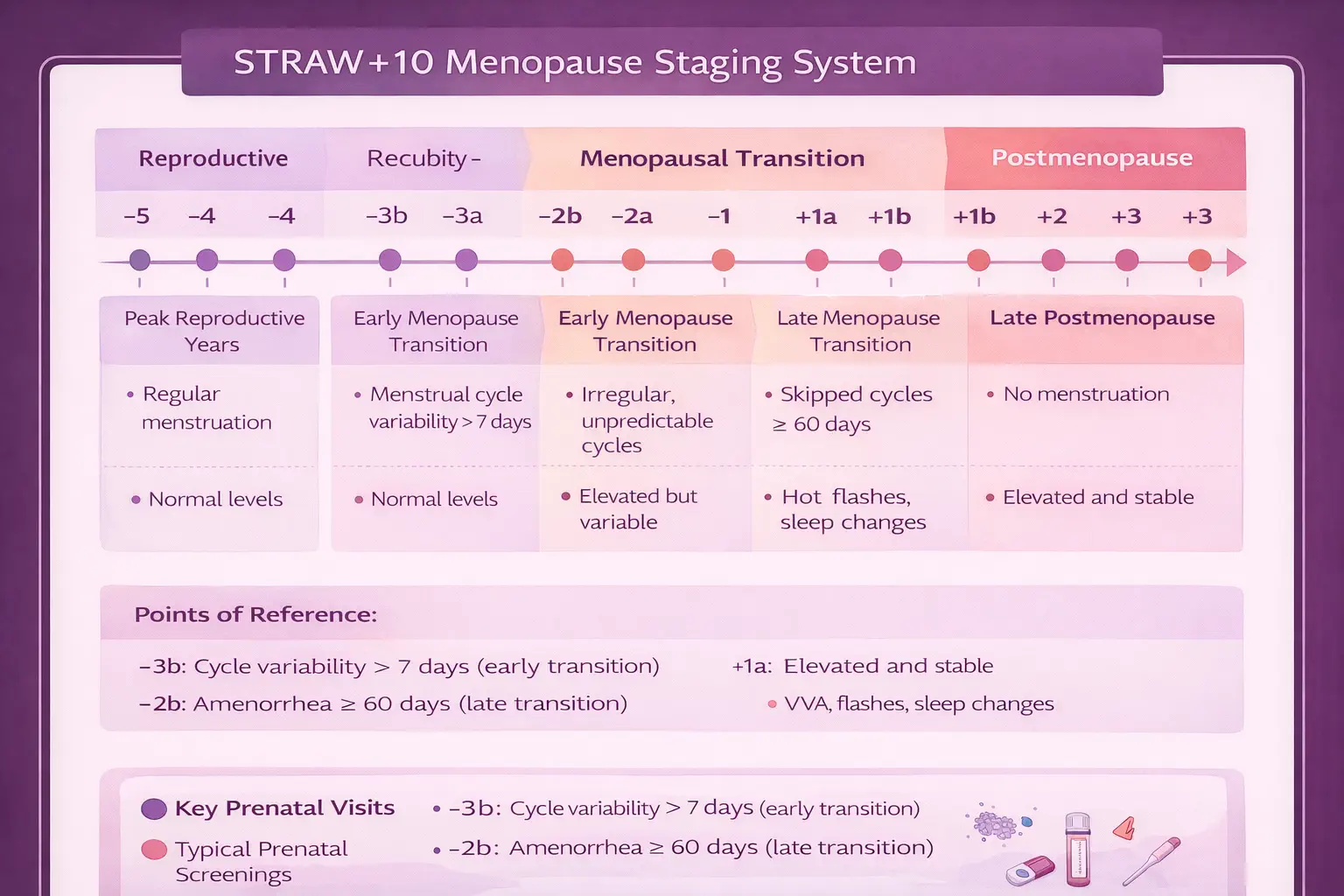
A comprehensive clinical resource for understanding menopause staging, HRT candidacy, risk-benefit analysis, treatment options, and monitoring protocols — grounded in current ACOG guidelines, the WHI reanalysis, the 2022 NAMS position statement, and the FDA’s 2025 labeling update.