Preeclampsia is a multisystem disorder of pregnancy characterized by new-onset
hypertension after 20 weeks of gestation combined with proteinuria or evidence
of end-organ dysfunction. It is one of the leading causes of maternal and perinatal
morbidity and mortality worldwide.
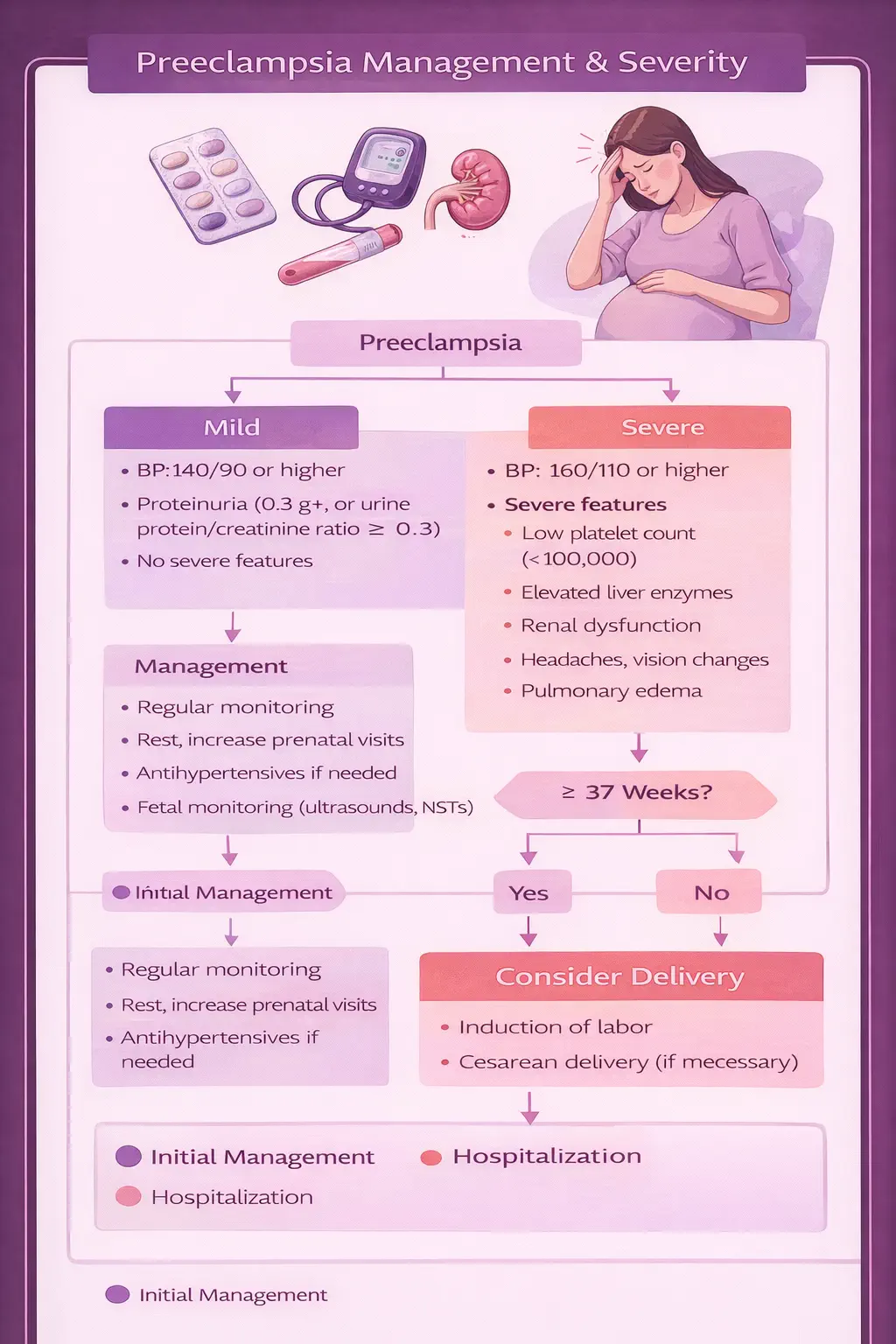
The diagnostic criteria are specific. Blood pressure must be ≥140 mmHg systolic
or ≥90 mmHg diastolic on two occasions at least four hours apart, occurring
after 20 weeks of gestation in a patient with previously normal blood pressure. This
hypertension must be accompanied by proteinuria (≥300 mg per 24-hour collection or a
protein-to-creatinine ratio ≥0.3) or, in the absence of proteinuria, evidence of
end-organ involvement: thrombocytopenia, renal insufficiency, elevated liver transaminases,
pulmonary edema, or new-onset cerebral or visual disturbances.
Prevalence estimates range from 3% to 8% of pregnancies worldwide, with
variation by population, access to prenatal care, and presence of underlying risk factors.
In the United States, the incidence has been increasing over recent decades, partly attributed
to rising rates of obesity, advanced maternal age, and chronic hypertension in the
reproductive-age population.
The clinical significance of preeclampsia cannot be overstated. Untreated or unrecognized
preeclampsia can progress to eclampsia (seizures), HELLP syndrome
(hemolysis, elevated liver enzymes, low platelets), placental abruption, acute kidney injury,
stroke, and maternal or fetal death. The only definitive treatment is delivery of the placenta,
which means that management decisions center on balancing maternal safety against fetal
gestational age and maturity.
This is why risk identification, prevention through aspirin prophylaxis, early
detection through structured prenatal monitoring, and evidence-based delivery timing
are the cornerstones of preeclampsia management. Each of these elements is discussed in
detail below.
For a comprehensive overview of how preeclampsia fits within the broader framework of
high-risk pregnancy care, see our
High-Risk Pregnancy Guide.